


Compounded Dental Anaesthetic

Recently I was sent a sample of 2% lignocaine in saline which had been put together by a pharmacist experienced in preparing medications from their constituent ingredients. The hope was that in doing so we could obtain a local anaesthetic that did not display the characteristic signs of complex chemistry and technology.
I was not optimistic as I had previously looked at a compounded version of procaine and it exhibited the same complex chemistry and crystal formation as the larger manufacturers but I was certainly happy to have another look. As expected the results were similar to previously. The pharmacist had added lignocaine powder with NaCl powder and distilled water in the right proportions to produce the desired concentration. However he or she had not manufactured any of the ingredients in house. They were not made ‘from scratch’.
I am certainly of the belief that I am seeing technology that self-assembles into complex structures from samples of dental anaesthetic. However, given that every one of the 15 or so samples I have looked at appears to show similar inexplicably complex chemistry it is worth considering where the components are actually synthesized.
It is possible, probably likely, that the bulk chemicals involved in manufacturing come from a small number of industry suppliers. These companies then supply the likes of Pfizer, Astra-Zenica, Sanofi, Septodont, Dentsply etc who use these raw materials to assemble, package and distribute their particular brands.
I have a number of videos of this process available on my website:

As well as previous posts:
Nanotechnology in Dental Anaesthetics
Nanotechnology in Dental Anaesthetics Part 2
Nanotechnology in Local Anaesthetics part 3 (closely followed by part 4)
Nanotechnology in local anaesthetic part 4 of many...
Dental Anaesthetic Differences
link to a video of Karl C. and myself discussing some of the processes in more detail
Compounded Sample lignocaine 2% in saline
Initial drop on the slide from a 1ml insulin syringe. Darkfield 25x magnification, showing the top of the drop.

video of the evaporative process:
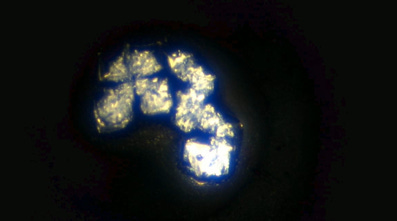
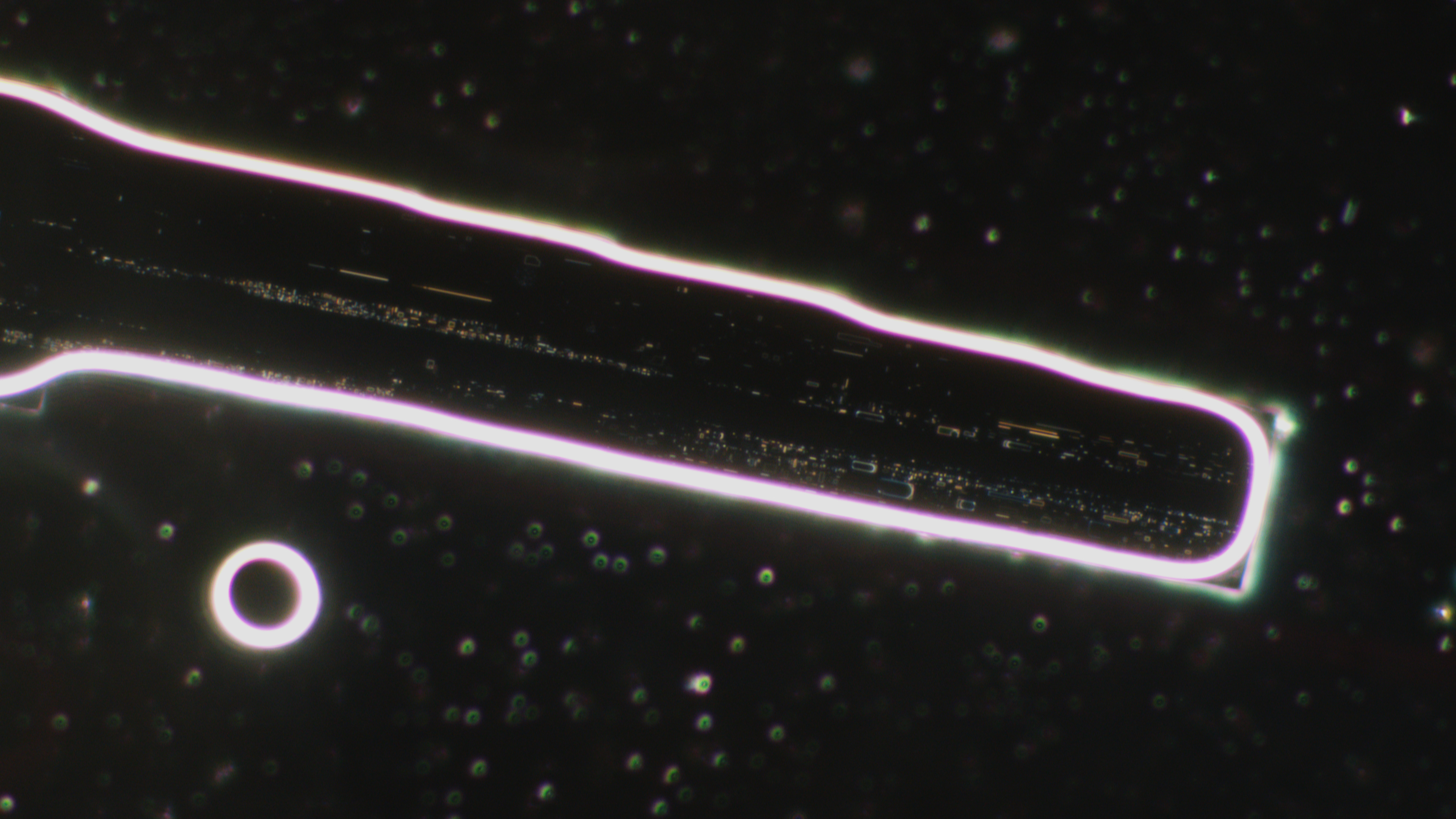
Crystal soon after it has formed. I would have taken a close up had I known I would use it later! Suffice to say it did not have most of the detail that you can see now.
Top left crystal 7 hours later:
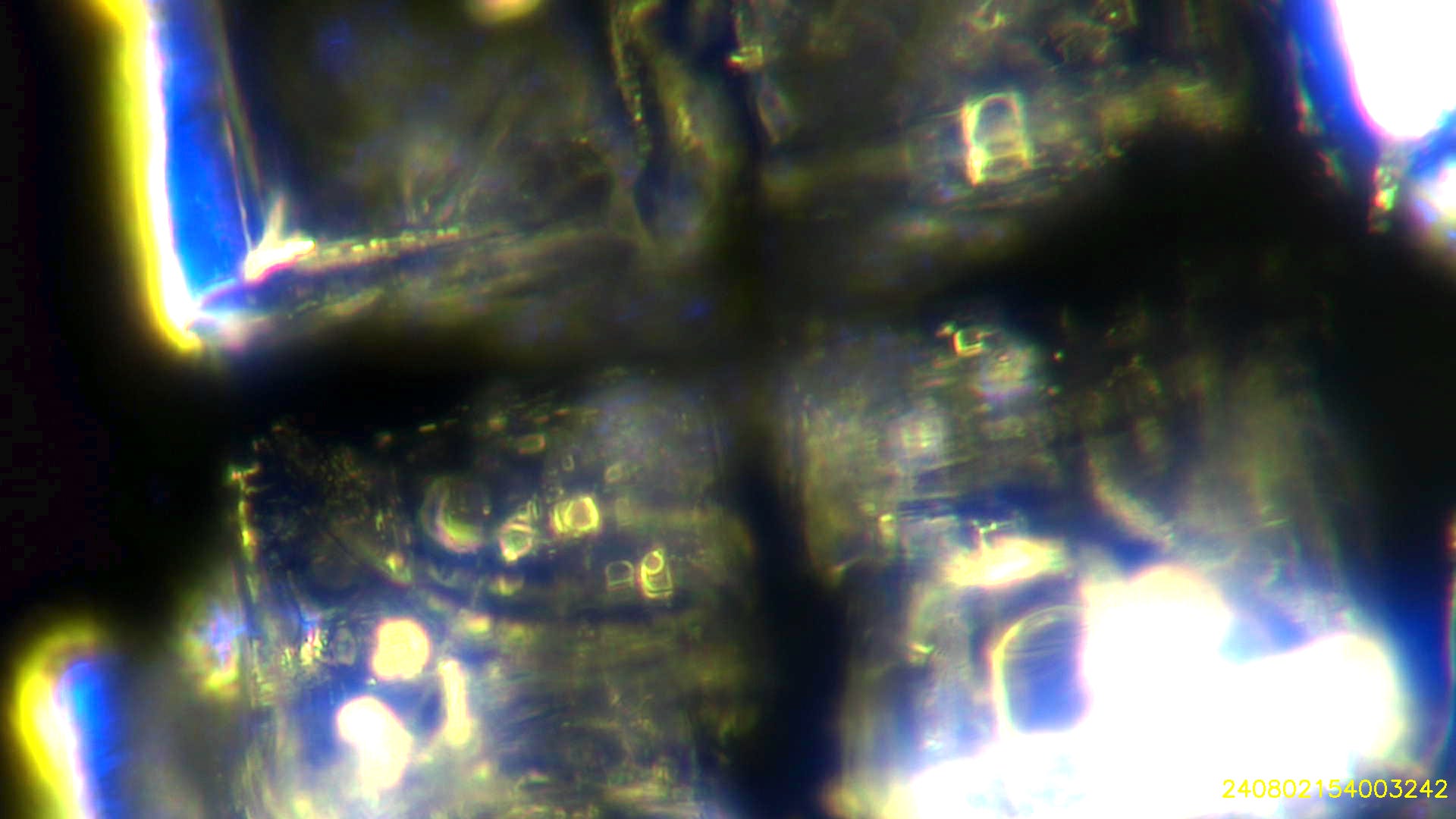

6 days later:


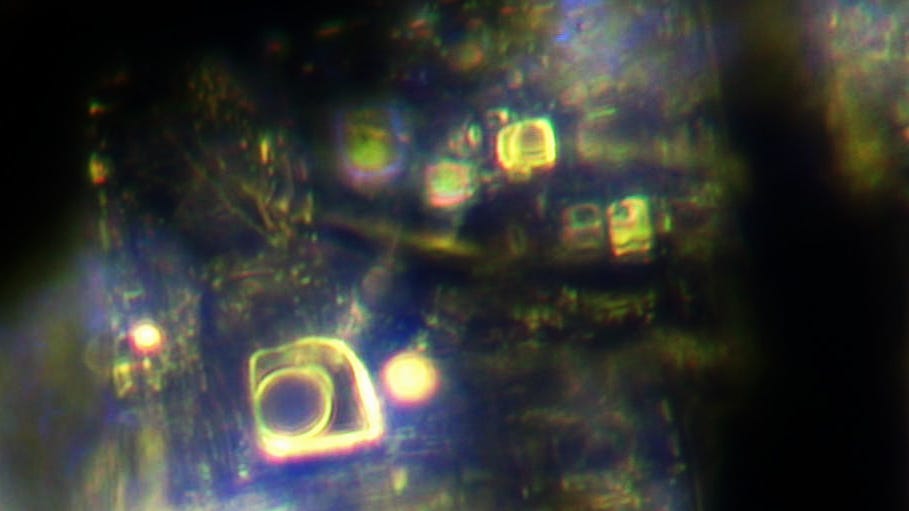

I also placed a drop of sample under a coverslip and this was one of the structures that developed after 5 days:
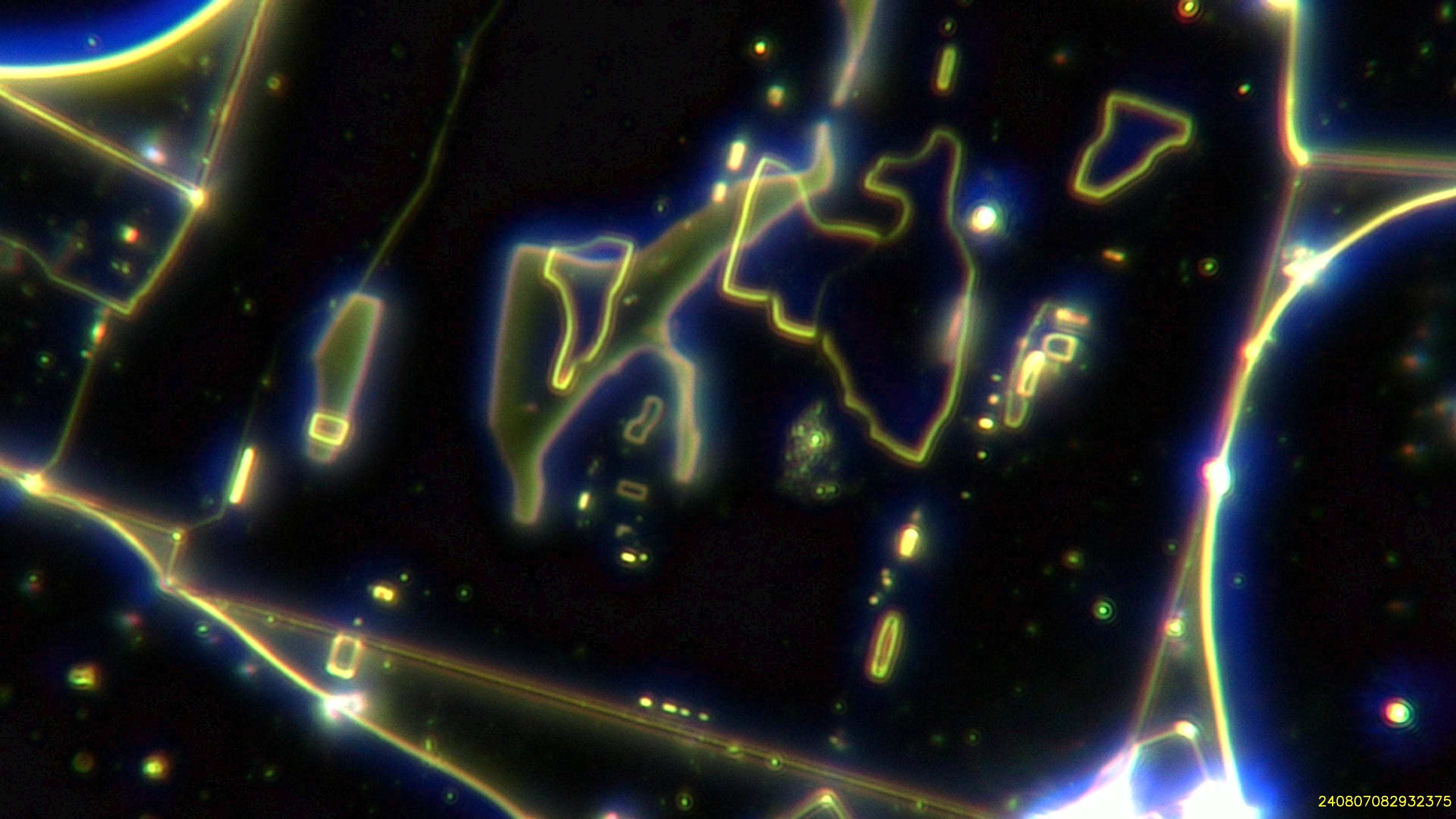
I have recently shown a few images that Louise C. has taken from a sample of Citanest dental anaesthetic under a coverslip. These images are definitely the best I have seen from structures that have developed in this way. I have spent many hours with Louise looking at these structures and I intend to showcase them in my next post. Here is a taste… :-)
Until then.
All the best for the end of the week.
David

All assistance much appreciated!

How to avoid such contamination? I rarely visit dentists but in past 10 years have one implant and 2 crowns. I so conscientious in drinking our own water from our falls in a pristine remote area, growing my own food, living consciously, growing and producing my own medical herbs, not visiting doctors or taking g drugs- and despite that I’m probably full of crystalline nano structures. And what can be done to remove these?
Thank you very much for this report, David.
In the US lignocaine is called lidocaine. They are identical chemical substances. These local anesthetics are widely used in pain prevention/relief for minor medical procedures throughout the world, either with epinephrine or without it. Intravenous lidocaine is used as a cardiac anti-arrythmia medication as well. Enough injectable medical products have already been examined microscopically to conclude that they are all intentionally tainted with micro/nanotechnology. It cannot be an accident or the result of poor manufacturing processes.
In some circumstances, one may choose to have an inhalant analgesic administered instead of a local injection. However, it is unknown whether these agents are free of contamination (perhaps someone has already tested them). There is the theoretical risk of it entering the blood stream through the pulmonary alveolar-capillary membrane which is even more direct than after a local injection. Therefore, someone who does this work, should obtain and examine a sample of one of the inhalant agents and report their findings.
The safest course of action is to completely avoid all injectable products unless absolutely necessary to either save one's life or prevent severe disabling pain/suffering when no other option is available.